Chris Thorman in an article on CCHIT and HITECH elaborates on the 'new issues' posed by HITECH.
For nearly four years, the Certification Commission for Health Information Technology (CCHIT) has been the lone entity recognized by the federal government to certify electronic health record systems. Since being named a recognized certifying body by Health and Human Services (HHS) in 2006, CCHIT has awarded certifications to nearly 200 EHR software products based on CCHIT’s standards of functionality, interoperability, usability and security.
However, CCHIT’s role in the EHR market is changing. The Office of the National Coordinator of Health IT (ONC) and the Center for Medicare & Medicaid Services (CMS) announced in early March 2010 that they would name more than one organization to certify EHR software, countering previous claims that CCHIT would become the sole certifying body.
Take the SURVEY
This points out the difficulties of having federal intrusion into the daily working of medical care and technology. He who signs the checks makes the rules. Not only is that a factor, but the rules change. Mandates are made and only a small percentage of these come to pass. Pilot studies and demonstration projects are planned, implemented, and studied. In a recent article
The Road to Wellville: Pilots and Demos?
By ROGER COLLIER
in The Health Care Blog he states:
"Just how important are all these pilots and demos? Harvard’s David Cutler, who served as a key advisor to the Obama administration in developing the reform strategy, clearly believes they are vital. Writing in the June Health Affairs, he stresses the need for rapid implementation of the pilots and demonstrations in order to help achieve eventual savings of “enormous amounts of money while simultaneously improving the quality of care..............The simple answer is that few providers will participate in a pilot or demonstration if it’s likely to cause their income to drop. As a result, CMS must attract “volunteers” with generous promises of shared savings or payments for additional services –essentially, bribes to compensate for lost revenue and the time-consuming process of dealing with CMS bureaucracy. So far, the bribes have outweighed the savings in almost every case. Worse still, and often overlooked in evaluations of pilots, participating providers are likely to be those most able to achieve savings—the “good guys,” rather than the typical—with resultant optimistic skewing of the results........................Results suggest that some of these programs may have modest effects on the quality of care and mixed impacts on Medicare costs, with most programs costing Medicare more than would have been spent had they not been implemented….
In almost all cases, the cost to Medicare of the intervention exceeded the savings generated by reduced use of inpatient hospitalizations and other medical services.”
Roger Collier was formerly CEO of a national health care consulting firm. His experience includes the design and implementation of innovative health care programs for HMOs, health insurers, and state and federal agencies. He is editor of Health Care REFORM UPDATE [reformupdate.blogspot.com]
Chris Thorman came to Software Advice after working in politics and with international non-profit organizations. He's originally from Kansas City and has been blogging about the Chiefs at ArrowheadPride.com since 2006. His articles have been mentioned in the New York Times, Wall Street Journal, Washington Post, Business Week, Sports Illustrated, ESPN and NFL.com. Currently, Chris resides in Austin, TX, with his wife Nichole and dog Winston.

























 ophthalmologists and others
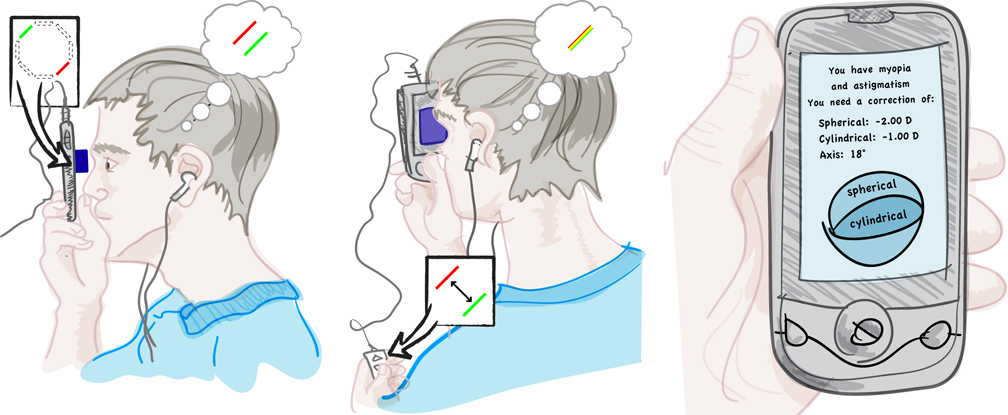
ophthalmologists and others  With this technique the autotracker is disengaged and the flying spot software is also disengaged. Pinhead or Patriot enhancements are also available. The laser has been certified as 'fair and balanced'
With this technique the autotracker is disengaged and the flying spot software is also disengaged. Pinhead or Patriot enhancements are also available. The laser has been certified as 'fair and balanced'
![[mark-sanford.jpg]](https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEjZDdpZ-8iIzvTHSq8VHC-8e1QAv1uRcM0y7rRozp76wQD8sv7shDtComNffPIjfqK0ocustfl7aP5E6kPkuzsyFq-dTvt0GcpvCr80CY6xvrjqagksn-nyUxH4WI8TECCwb9VPT5c6oWs/s1600/mark-sanford.jpg) Lasik offers a free trip to Argentina for both the procedure and post operative visits. An option is a free escort service.
Lasik offers a free trip to Argentina for both the procedure and post operative visits. An option is a free escort service. offers a free trip to the United States with a refundable return ticket to Afghanistan (cannot be transferred). The procedure is pre-approved and in accordance with all DOD regulations, and is free of charge.
offers a free trip to the United States with a refundable return ticket to Afghanistan (cannot be transferred). The procedure is pre-approved and in accordance with all DOD regulations, and is free of charge.