This is the first in a series of articles on changes in education, the physician workforce, and what is driving changes.

Many studies have been done to analyze the physician/population ratios in different areas of the United States. In addition to their being an overall shortage of physicians, there is a disparate imbalance of primary care physicians (formerly called family doctors and/or general practitioner) and specialty physicians. This general statistic does not delve into specific oversupply of specific specialties. In some cases there is a severe shortage of psychiatrists, and mental health professionals. The statistics also do not account for physicians who function in a primary care role, but are not statistically accounted for, as such. For instance, Ob/Gyn, Moonligthing resident physicians who staff ED and Urgent care centers, Pediatricians, some general internal medicine physicians who function in a dual role as a PCP and specialist. Many women use their Ob/Gyn specialist as a PCP.
In the last several decades the number of female physicians accepted into medical school has increased. Women are faced with a difficult choice, biological imperatives and the very real responsibility of medical practice. For that reason many select a specialty with controlled hours, or a hospital specialty such as radiology or anesthesiology, dermatology, not primary care. For those who do select primary care their careers are punctuated by pregnancy, family needs, and often premature retirement, or finding a non-clinical career.
Karen Sibert,M.D. (who is an anesthesiologist) writes in the New York times,
“I’m a doctor and a mother of four, and I’ve always practiced medicine full time. When I took my board exams in 1987, female doctors were still uncommon, and we were determined to work as hard as any of the men.

Today, however, increasing numbers of doctors — mostly women — decide to work part time or leave the profession. Since 2005 the part-time physician workforce has expanded by 62 percent, according to recent survey data from the American Medical Group Association, with nearly 4 in 10 female doctors between the ages of 35 and 44 reporting in 2010 that they worked part time. .
About 30 percent of doctors in the United States are female, and women received 48 percent of the medical degrees awarded in 2010. But their productivity doesn’t match that of men. In a 2006 survey by the American Medical Association and the Association of American Medical Colleges, even full-time female doctors reported working on average 4.5 fewer hours each week and seeing fewer patients than their male colleagues. The American Academy of Pediatrics estimates that 71 percent of female pediatricians take extended leave at some point — five times higher than the percentage for male pediatricians.
Today 53 percent of family practice residents, 63 percent of pediatric residents and nearly 80 percent of obstetrics and gynecology residents are female.
The uniformed medical services have PCPs that are not available to the general public unless they moonlight in an outside practice, hospital, or urgent care center. The statistics do not account for these PCPs.
Other PCPs who are not counted are optometrists, chiropractors, or nurse practitioners working in retail clinics.
Many other specialists will function as a PCP on many occasions to serve their patients for minor illnesses, such as prescription refills, outside of their specialty certification.
A contributing cause to the relative deficiency in PCP accessibility is the increasing rigidity and bureaucracy of the medical system in the United States. Certain medico-legal issues also preclude and diminish the ability to practice general medicine by a threat of litigation when practicing outside the bounds of specialty certification.
The Association of American Medical Colleges estimates that, 15 years from now, with the ranks of insured patients expanding, we will face a shortage of up to 150,000 doctors. As many doctors near retirement and aging baby boomers need more and more medical care, the shortage gets worse each year.

The short answer is yes there is a relative shortage of PCPs, however there is no shortage of specialty physicians. Perhaps there is an imbalance and availability of specialists. Many of the factors are aggravated by what happens between a medical student’s enrollment in medical school, and their graduation from school, or during the training years.
This gap is especially problematic because women are more likely to go into primary care fields — where the doctor shortage is most pronounced — than men are. Today 53 percent of family practice residents, 63 percent of pediatric residents and nearly 80 percent of obstetrics and gynecology residents are female.
Medical licensure by states offers a license to practice general medicine, and in fact does not restrict in most cases what type of medicine a physician practices. Specialty care is regulated mostly by hospital credentialing authority for procedures, and departmental classification by medical staff regulations and bylaws overseen by the hospital administration.
Recently the public’s attention has been brought to the expenses of a medical education, and the economics of 150,000 to 200,000 dollars borrowed to pay for it by a student. Some would say this is an investment in the student’s future, however there are burdens also on society. While it is an economic boon and cash cow for banks regarding interest, it produces another parasitic industry, and more bureaucracy.
Dr Sibert goes on to say,
“Medical training is not available in infinite supply, if it were there would be graduates to replace or supplement those who work part-time, however, can only afford to accept a fraction of students who apply.
An even tighter bottleneck exists at the level of residency training. Residents don’t pay tuition; they are paid to work at teaching hospitals. Their salaries are supported by Medicare, which pays teaching hospitals about $9 billion a year for resident salaries and teaching costs as well as patient care.
In 1997, Congress imposed a cap on how many medical residencies the government could subsidize as part of the Balanced Budget Act. Last year, the Senate failed to pass an amendment to the health care bill that would have created thousands of new residency positions. Even if American medical schools could double their graduating classes, there wouldn’t be additional residency positions for the new doctors. Federal and state financing to expand medical education will be hard to find in today’s economic and political climate.”
Policy makers could encourage more doctors to stay in the profession by reforming the malpractice system to protect them from frivolous lawsuits, safeguarding their pay from further Medicare cuts and lightening the burden of bureaucratic regulations and paperwork.
PCPs carry a disproportionate share of paper-work and also acting as the gatekeeper for specialty referrals, insurance company authorizations, telephone work (none of which is reimbursable, yet takes up at least 10-25% of the daily workload).
Physicians defer saving money during their early years meeting this financial obligation, at the same time deferring home ownership. Many are in their late 20s and early 30s before they have disposable income to meet loan payments. In some cases interest accrues until payments are begun. All physicians are aware of the conundrum, increasing tuition, living expenses, deferred adulthood and dependency upon parents and relatives. Few would make it through the system without family assistance in some form.
The emotional toll of these circumstances cannot be overestimated for medical students and their families. Unlike PhD candidates who receive fellowship grants medical students have far fewer institutional or federal grants, unlike NIH grants, or federal NSF grants.
The deferment of savings also has a severe effect on eventual retirement for the early years the lack of the most powerful investment tool (the compound interest curve of savings, or even other investments is negated).
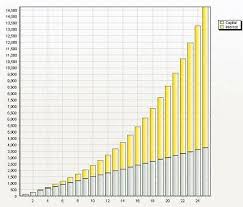
Compound Interest Curve is exponential
Lack of any saving during the first ten years of adult life, between age 30 and 40 years of age will later effect a physicians life, and statistics reveal there are many physicians who cannot retire or do so in poverty, totally dependent on social security benefits.
The problems are serious, and not isolated from the many challenges of medical practice. Physicians have been left out of the planning process, most practitioners are now isolated from academic medicine and no longer are directly involved in training new physicians. Most of us receive requests from alumni organizations asking for donations, bequeaths and scholarship funding for individual medical students.











