Normally I post articles on health reform, and information technology.
However today I was in the process of preparing examination questions for board preparation for the American Board of Ophthalmoloogy, and came upon this poignant observation by a medical resident.
It also points out the importance of tight glycemic control for diabetic patients.
Insight
Elizabeth B. Gay, MD
Charlottesville, Virginia
eg3d@hscmail.mcc.virginia.edu
JAMA. 2010;303(3):205.
The right eye bleeds on a Wednesday morning. I am walking to clinic, heading up the hill on 97th Street. For a moment, I imagine the dark spot is some trick of light and shadow. But it grows before me, spreading outward from its center, forming a web across my vision.

I know the correct medical language—vitreal hemorrhage—

but can only think: My eye is bleeding. The growing web floats across the world, almost beautiful if I weren't so afraid. I had a laser treatment on this eye two days ago, to prevent fragile new vessels from bleeding.

The right eye has always been the good eye; the left has been bleeding for a year, despite more laser sessions than I can count. I know I will need a vitrectomy


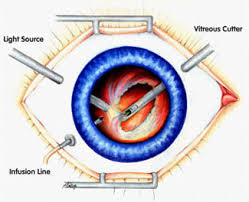
on the left eye, but I was counting on the right. This bleeding is the result of diabetic retinopathy and so particularly painful because it is in part my fault. Previously obsessive about my blood glucose, during my intern year of medicine residency, exhilarated and exhausted by the rigors of training, I struggled for reasonable control. And I let myself be 180 rather than 80, given the inconvenience of being low. My blurry vision feels like punishment, and usually I believe it's deserved.
I keep walking to clinic because there's nothing to be done right away—I can't have more laser after only two days. It is a perfect fall day, clear and sunny, but it is disappearing under a growing darkness. I am afraid that I will never again experience this sharp morning light, that I will always remember this morning as a moment of loss. Practical concerns add to my sense of despair: I’m on call for the ICU in two days, and the vision in my left eye is already blurry. I need the right eye to function. Of course this need doesn't matter, the body impervious to my panicked mind.
Clinic is chaotic as usual, and I abandon any attempt to read scribbled chart notes. On the computer I enlarge the font, grateful for modern technology. And most of what I need to know, patients tell me. Somehow the day goes on. This is how it's done, this is how people cope with illness. You go on because there is no choice. You go to work and do the best you can. Medicine is a good job because it's easy to forget yourself. Working in the ICU on Thanksgiving Day, I tell myself that the threat of blindness is less than what my patients face. I hold in my mind images of bravery offered to me every day, families who pull together to make unbearable decisions about the end of life, patients who somehow find pleasure in being an "interesting patient." But I can't quite convince myself. I would prefer the threat of death to that of blindness. Reading for me seems as essential as breathing, as impossible to live without. And then there is this: What if I can't do the job I’ve been working toward for eight years? But it is more than that because it's somehow become more than a job: it's become who I am. I am afraid that if I can't be a physician, I will lose my self.
I am saved by medicine after all, by a superb ophthalmologist and his colleague who skillfully remove the vitreous of my left, then my right eye. After each operation I must keep my head parallel to the floor for three days. This is the posture of defeat, the posture of despair, and it is hard not to feel it. The metaphor of the darkest hour becomes real for me in those first days after the second operation, both eyes recovering, a time when faces are blurry and indistinct. I am acutely aware of time as a palpable dimension, made to pass by music and books on tape. My vision slowly improves, leaving me able to do my job, and determined never to complain about having to do it, never to whine about returning in the middle of the night to the ICU, never to complain about a presentation or journal club. And every morning I am both grateful to be able to see and afraid it might not last. I am like my patients, like all survivors of illness, left with gratitude and uncertainty, wonder and fear.
A Piece of My Mind Section Editor: Roxanne K. Young, Associate Senior Editor.